Researchers Raise Methodology Concerns Over Teen Energy Drink Heart Study
A new letter challenges the methodology of the EDKAR study on energy drinks and cardiovascular risk in adolescents, raising questions about data interpretation.
A group of pediatric cardiologists at Ludwig Maximilian University in Munich has published a critique of the EDKAR study, a recent piece of research on chronic energy drink consumption and cardiovascular risk in teenagers. Their letter, published in the European Journal of Epidemiology, doesn't dispute the original study's data -- it disputes whether the study was designed well enough to draw conclusions from it.[1]
Before getting into the critique, it's worth being clear on what the original study actually found, because it didn't get much honest media coverage:
Background on the EDKAR Study: What Was Found
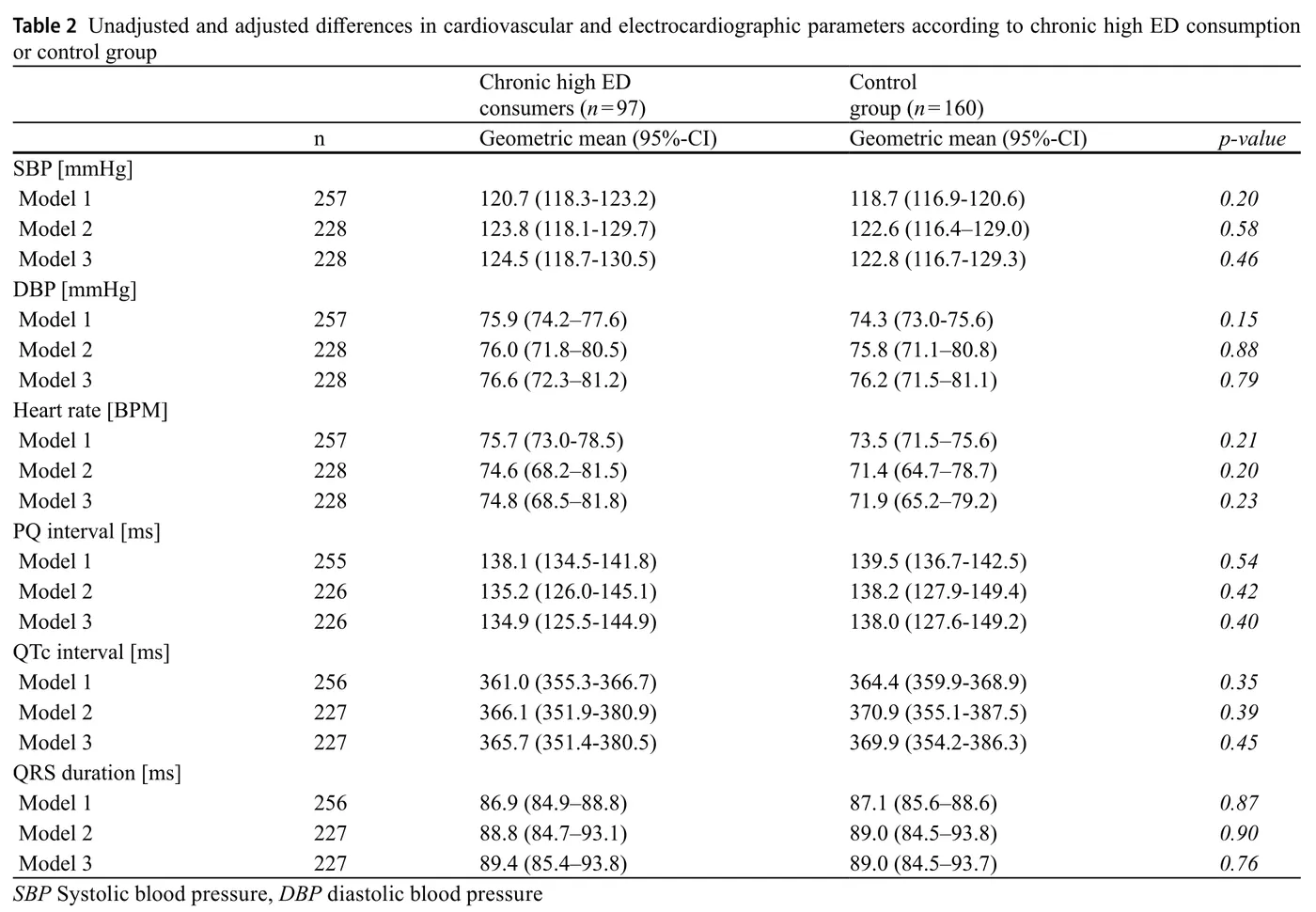
The EDKAR study ran full cardiac workups on 97 teenagers who had consumed energy drinks heavily (four or more days per week for at least a year, at more than 3mg caffeine per kg of bodyweight per day) and compared them to 160 controls. Researchers measured blood pressure, heart rate, standard ECG parameters, and a comprehensive battery of echocardiographic measurements.[2]
The result: no statistically significant differences in any cardiac parameter.[2] Not heart rate, not systolic or diastolic blood pressure, not ECG intervals, not echocardiographic measures. The p-values across the board ranged from 0.15 to 0.90 (nowhere close to significance) and held up across multiple sensitivity analyses at even higher consumption levels.
That's the headline finding... although it didn't make headlines. It wasn't a warning signa nor a subtle red flag. Basically, just a null result across comprehensive cardiac testing.[2]
The critics are raising methodological concerns, but it's important to understand they're pushing back on a study that found nothing alarming, not one that found harm. However, a great deal did report having experienced palpitations and poor sleep at some point, and there were some trends towards significance that led to some debate.
The Confounding Problem
The Munich team's most direct criticism is that the two groups weren't matched at baseline. Chronic high energy drink consumers in the EDKAR study were older, had higher BMIs, and reported dramatically more tobacco, alcohol, and marijuana use than controls. Over 50% of the heavy ED group smoked, compared to under 2% of controls. More than half slept fewer than six hours on weeknights, versus 13% of controls.
This makes sense, since older adolescents will be more likely to drink energy drinks than younger ones (although nobody under the age of 18 should ideally have any), which leads to increases in other at-risk behaviors. But the data didn't account for that.
This is a definite limitation. When you're trying to isolate what energy drinks do to cardiovascular health, having your high-consumption group also smoke more, drink more alcohol, and sleep significantly less makes attribution nearly impossible. The EDKAR authors acknowledged this, and their adjusted statistical models did account for these factors, but confounders this large are hard to fully correct for in a cross-sectional study.
The letter also raises a timing issue: cardiovascular measurements may have been taken after an energy drink pause, since teenagers visiting a university hospital would likely skip their morning drink. If so, researchers may have been measuring trough values rather than real-world cardiovascular status. The study didn't specify when participants last consumed an energy drink before their examination.
Measurement Tools and Reference Standards
Beyond confounding, the Munich team raises two technical objections.
-
First, a standard 12-lead ECG has limits for assessing arrhythmia risk. They argue a 24-hour Holter ECG would give a more reliable picture of any irregular rhythms that might appear during or after energy drink consumption. The same applies to blood pressure: a single-point measurement is noisier than 24-hour ambulatory monitoring.
-
Second, the EDKAR study used adult cardiovascular reference values to interpret measurements in a teenage population. Pediatric cardiology uses age-, sex-, height-, and weight-adjusted reference ranges for the same parameters -- chamber dimensions, wall thickness, echocardiographic values. Using adult benchmarks on adolescents can misclassify normal teenage physiology. The Munich team wants the data reinterpreted using pediatric Z-scores before any conclusions are drawn.
Reading Trends Into Non-Significant Data
The most notable part of the critique is where the Munich team argues that certain non-significant trends in the EDKAR data deserve more attention. They point to diastolic blood pressure appearing to increase across consumption groups, and septal wall thickness edging upward, as early indicators of possible left ventricular afterload changes.
These trends were present in the raw data, but weren't statistically significant after adjustment. The EDKAR authors ran their numbers through multiple models and attempted corrections across 216 tests. Yet nothing crossed the significance threshold.
Pointing to non-significant directional trends as "worrisome findings" is a different interpretive standard than the one the original study applied. That doesn't make the Munich team wrong to flag them for future research -- subtle signals in young populations are worth tracking. But framing non-significant trends as evidence of harm goes further than the data supports.
What to Make of the Dose Data
The letter also notes that the EDKAR study buries dose information in an appendix rather than presenting it in the main tables. Body weight, relative caffeine intake per kilogram, and absolute energy drink volumes are missing from the primary data. The Munich team estimates that, based on appendix data and average bodyweight for an 18-year-old, some participants were consuming around 400mg to 600mg of caffeine daily.
For context: EFSA considers up to 400mg per day of no concern for healthy adults chronically, with up to 600mg regarded as generally mild and reversible in its cardiovascular effects.[1] The EDKAR participants were teenagers, not adults, so those adult thresholds don't apply directly -- and the Munich team argues they shouldn't be extended to adolescents. That's fair. But it's worth noting these doses aren't far outside ranges that existing adult research considers manageable.
What This Doesn't Mean
None of this resolves what chronic, high-dose energy drink consumption does to a developing cardiovascular system over years. The EDKAR study was cross-sectional, so it can't speak to long-term effects. The Munich team's concern about subtle trends becoming "more relevant after several years" is worth taking seriously even if the current data don't show it.
But the honest read on EDKAR is that a well-designed (if imperfect) study put teenagers with serious energy drink habits through comprehensive cardiac testing and found no significant abnormalities.[2] The critique that followed raises methodological concerns worth addressing in future research, but it doesn't retroactively turn a null result into evidence of harm.
For adults, the picture on moderate-to-high energy drink consumption remains what it's been: manageable at reasonable doses for healthy people, with real concerns at extremes. For teenagers, the data is still thin enough that caution makes sense -- not because EDKAR found problems, but because it hasn't been around long enough to know.
Subscribe to Bevlab's newsletter at the bottom of this page, we'll continue watching this story as the research develops.
References
- Haas NA et al. "Re: 'Chronic high consumption of energy drinks and cardiovascular risk in adolescents - results of the EDKAR study'." European Journal of Epidemiology, 2026. https://link.springer.com/article/10.1007/s10654-025-01339-1
- Menzel et al. "Chronic high consumption of energy drinks and cardiovascular risk in adolescents -- results of the EDKAR-study." European Journal of Epidemiology, 2025. https://link.springer.com/article/10.1007/s10654-025-01292-z